



1. Introduction
| 1. Recognizing that civil information includes both positive and negative content, we consider the varying positive and negative correlations between official and civil information. | |
| 2. We analyze the mutual coupling effect between epidemic transmission and information from different sources, including both official and civil channels. Specifically, we assess how varying correlations between these sources influence epidemic dynamics, emphasizing that individuals in infected and susceptible states respond differently to official and civil information. | |
| 3. Due to the prevalence of online rumors, individuals exhibit caution in adopting civil information. During the dissemination of civil information, individuals assess civil information based on their perceived infection risk and the degree of alignment between the civil information and official narratives before deciding whether to adopt it. | |
| 4. Based on the three-layer coupled transmission model we constructed, the state transition process of the model is analyzed using the Micro Markov Chain Approach (MMCA) to derive the epidemic threshold, and finally simulation analysis is conducted to validate the model’s effectiveness. |
2. The three-layer coupled model
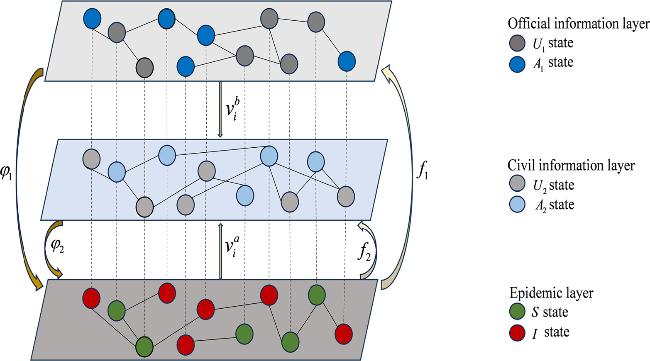
Figure 1. Structure of the three-layer ${U}_{1}{A}_{1}{U}_{1}-{U}_{2}{A}_{2}{U}_{2}-SIS$ propagation network framework. |

Figure 2. Propagation process of the official information diffusion. The dark blue circle represents individuals who believe in official information, while the dark gray circles represent individuals unaware of official information. |
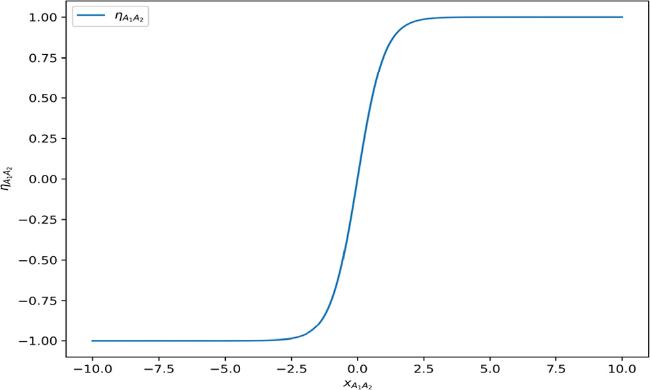
Figure 3. The impact of the correlation between different information on information recipients. |

Figure 4. Propagation process of the civil information diffusion. The light blue circle represents individuals who believe in civil information, while the light gray circles represent individuals unaware of civil information. |

Figure 5. Propagation process of the epidemic transmission. The green and red circles represent the susceptible and infected states in the SIS model, which appear in the epidemic layer. |
3. The theoretical analysis based on MMCA
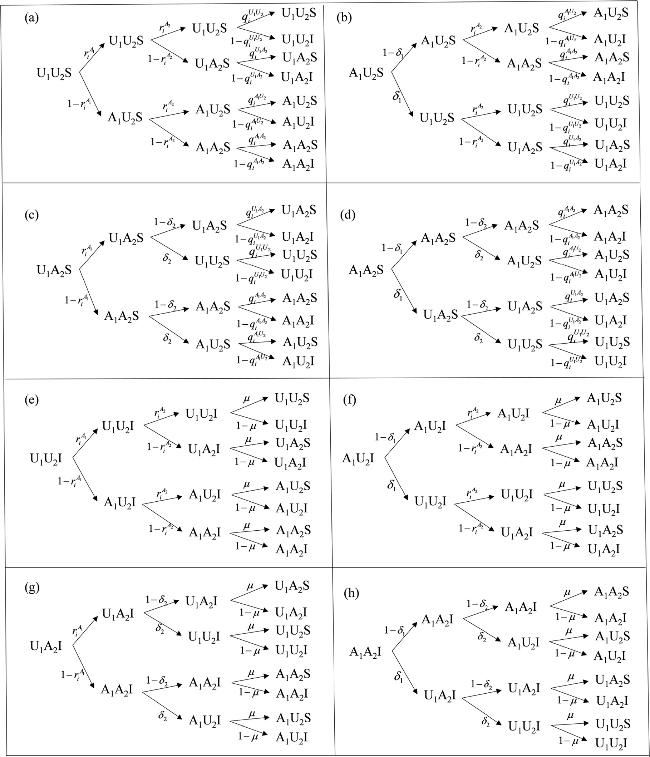
Figure 6. Probability tree of the eight possible node states in the model. |
4. The numerical simulations
4.1. The impact of information correlation on epidemic transmission
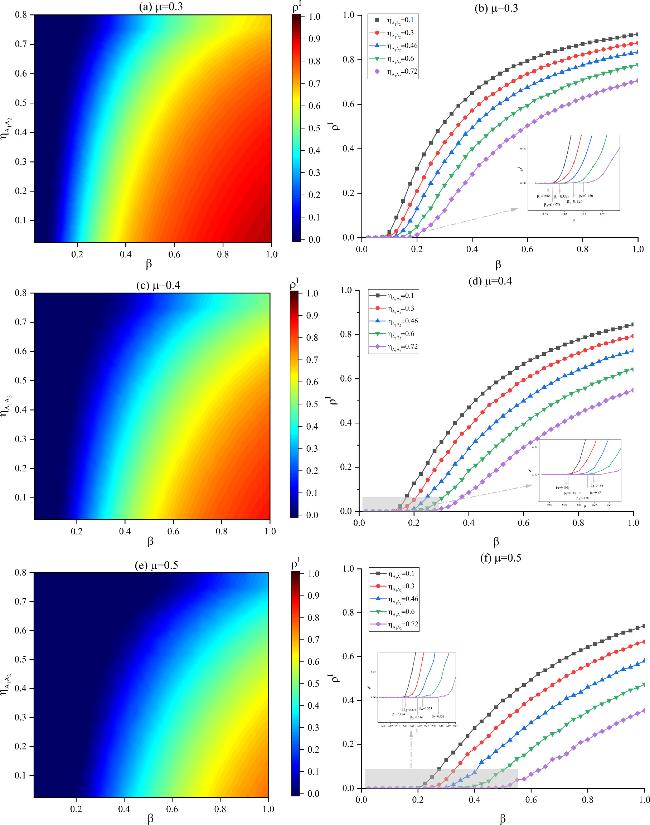
Figure 7. Epidemic scale as a function of the basic infection rate and the impact of different positive correlation ${\eta }_{{A}_{1}{A}_{2}}$. The basic recovery rate in different subplots is set as follows: (a) and (b) $\mu =0.3$, (c) and (d) $\mu =0.4$, (e) and (f) $\mu =0.5$. Other parameters are set as follows: $\lambda =0.2$, $f=0.6$, $K=0.3$, ${\omega }_{2}=0.5$, ${\delta }_{1}=0.4$, ${\delta }_{2}=0.5$, ${\varphi }_{1}=0.4$, ${\varphi }_{2}=0.8$. |
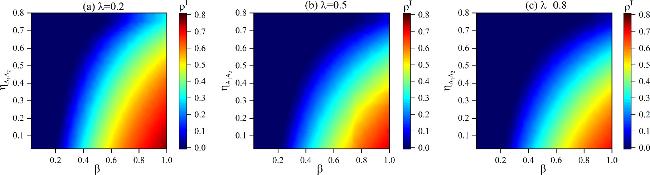
Figure 8. The influence of $\beta $ and the impact of positive correlation ${\eta }_{{A}_{1}{A}_{2}}$ on ${\rho }^{I}$. The transmission rate of official information in different subplots is set as follows: (a) $\lambda =0.2$, (b) $\lambda =0.5$, (c) $\lambda =0.8$. Other parameters are set to be $f=0.6$, $K=0.3$, ${\omega }_{2}=0.5$, ${\delta }_{1}=0.4$, ${\delta }_{2}=0.5$, $\mu =0.5$, ${\varphi }_{1}=0.4$, ${\varphi }_{2}=0.8$. |
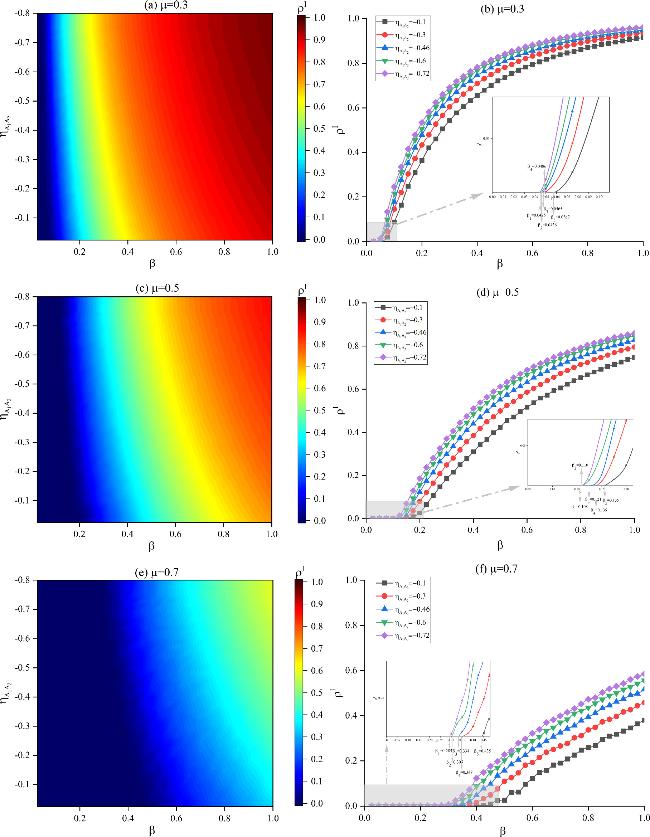
Figure 9. Epidemic scale as a function of the basic infection rate and the impact of different negative correlation ${\eta }_{{A}_{1}{A}_{2}}$. The basic recovery rate in different subplots is set as follows: (a) and (b) $\mu =0.3$, (c) and (d) $\mu =0.5$, (e) and (f) $\mu =0.7$. Other parameters are set as follows: $\lambda =0.5$, $f=0.6$, $K=0.3$, ${\omega }_{2}=0.5$, ${\delta }_{1}=0.4$, ${\delta }_{2}=0.5$, ${\varphi }_{1}=0.4$. |
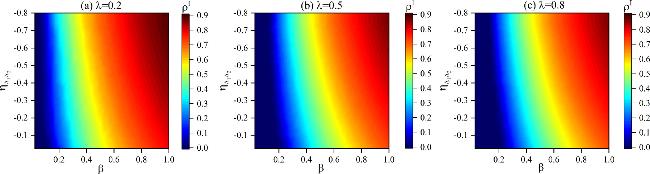
Figure 10. The influence of $\beta $ and the impact of negative correlation ${\eta }_{{A}_{1}{A}_{2}}$ on ${\rho }^{I}$. The transmission rates of official information in different subplots are set as follows: (a) $\lambda =0.2$, (b) $\lambda =0.5$, (c) $\lambda =0.8$. Other parameters are set to be $f=0.6$, $K=0.3$, ${\omega }_{2}=0.5$, ${\delta }_{1}=0.4$, ${\delta }_{2}=0.5$, $\mu =0.5$, ${\varphi }_{1}=0.4$. |
4.2. The impact of civil information adoption preference on epidemic transmission
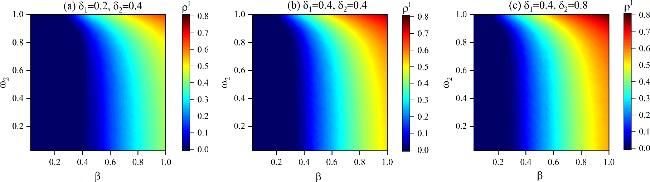
Figure 11. The influence of $\beta $ and ${\omega }_{2}$ on ${\rho }^{I}$. The information forgetting rates in different subplots are set as follows: (a) ${\delta }_{1}=0.2,\,{\delta }_{2}=0.4$, (b) ${\delta }_{1}=0.4,\,{\delta }_{2}=0.4$, (c) ${\delta }_{1}=0.4,\,{\delta }_{2}=0.8$. Other parameters are set as follows: ${\eta }_{{A}_{1}{A}_{2}}=0.46$, $\lambda =0.3$, $K=0.1$, $f=0.9$, $\mu =0.5$, ${\varphi }_{1}=0.4$, ${\varphi }_{2}=0.6$. |
4.3. The effect of interlayer mutual coupling on epidemic transmission
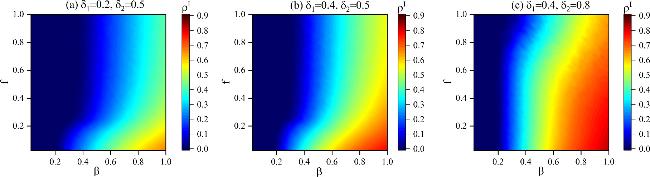
Figure 12. The function of epidemic scale ${\rho }^{I}$ with basic infection rate $\beta $ and different information decay coefficients $f$. The information forgetting rates in different subplots are set as follows: (a) ${\delta }_{1}=0.2,\,{\delta }_{2}=0.5$, (b) ${\delta }_{1}=0.4,\,{\delta }_{2}=0.5$, (c) ${\delta }_{1}=0.4,\,{\delta }_{2}=0.8$. Other parameters are set as follows: ${\eta }_{{A}_{1}{A}_{2}}=0.46$, $\lambda =0.2$, $K=0.3$, ${\omega }_{2}=0.5$, $\mu =0.5$, ${\varphi }_{1}=0.4$, ${\varphi }_{2}=0.8$. |
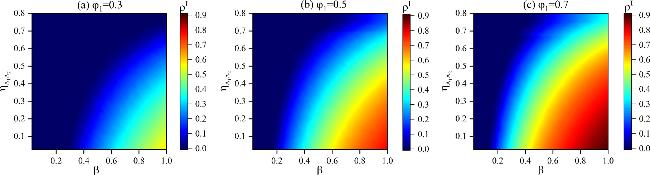
Figure 13. The function of epidemic scale ${\rho }^{I}$ with basic infection rate $\beta $ and different positive correlation ${\eta }_{{A}_{1}{A}_{2}}$. The decay factors in different subplots are set as follows: (a) ${\varphi }_{1}=0.3$, (b) ${\varphi }_{1}=0.5$, (c) ${\varphi }_{1}=0.7$. Other parameters are set as follows: $\lambda =0.5$, $f=0.6$, $K=0.3$, ${\omega }_{2}=0.5$, ${\delta }_{1}=0.4$, ${\delta }_{2}=0.5$, $\mu =0.5$, ${\varphi }_{2}=0.8$. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
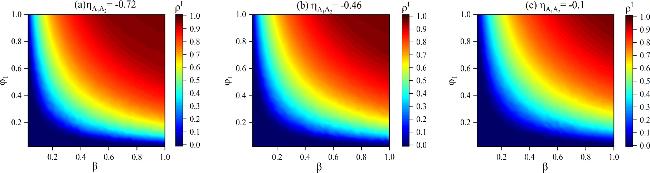
Figure 14. The function of epidemic scale ${\rho }^{I}$ with infection probability $\beta $ and attenuation factor ${\varphi }_{1}$. The negative correlation in different subplots is set as follows: (a) ${\eta }_{{A}_{1}{A}_{2}}=-0.72$, (b) ${\eta }_{{A}_{1}{A}_{2}}=-0.46$, (c) ${\eta }_{{A}_{1}{A}_{2}}=-0.1$. Other parameters are set as follows: $\lambda =0.2$, $f=0.3$,$K=0.3$, ${\omega }_{2}=0.5$, ${\delta }_{1}=0.4$, ${\delta }_{2}=0.5$, $\mu =0.5$. |
5. Conclusion
| 1. Strengthening the positive correlation between official and civil information can increase the epidemic threshold and reduce the scale of the epidemic, whereas a stronger negative correlation amplifies the scale of epidemic transmission. However, the impact of the negative correlation between official and civil information on the epidemic threshold and transmission scale is weaker than that of the positive correlation. Therefore, strengthening the dissemination of official information and actively adopting positive civil information closely aligned with official guidance is essential for epidemic control. | |
| 2. When adopting civil information, individuals should more thoroughly assess infection risks based on their personal circumstances and the surrounding environment to determine whether to adopt the information, thereby contributing to more effective disease control. | |
| 3. Enhancing the ability of infected individuals to accurately understand official information is crucial for effective epidemic management and ensuring adherence to public health guidelines. |